


When a patient mentions they’ll need a follow-up in a few weeks, the natural time to book it is right then, while they’re still in front of you. However, you’re not always at your desk to create the appointment straight away.
Today, we’re giving you that ability with appointment scheduling in Atlas.md Mobile, so you can create a new appointment directly on your phone, no matter where you are. Booking takes a few taps and happens without interrupting the visit.
Schedule Your Patient’s Next Visit From Your Phone
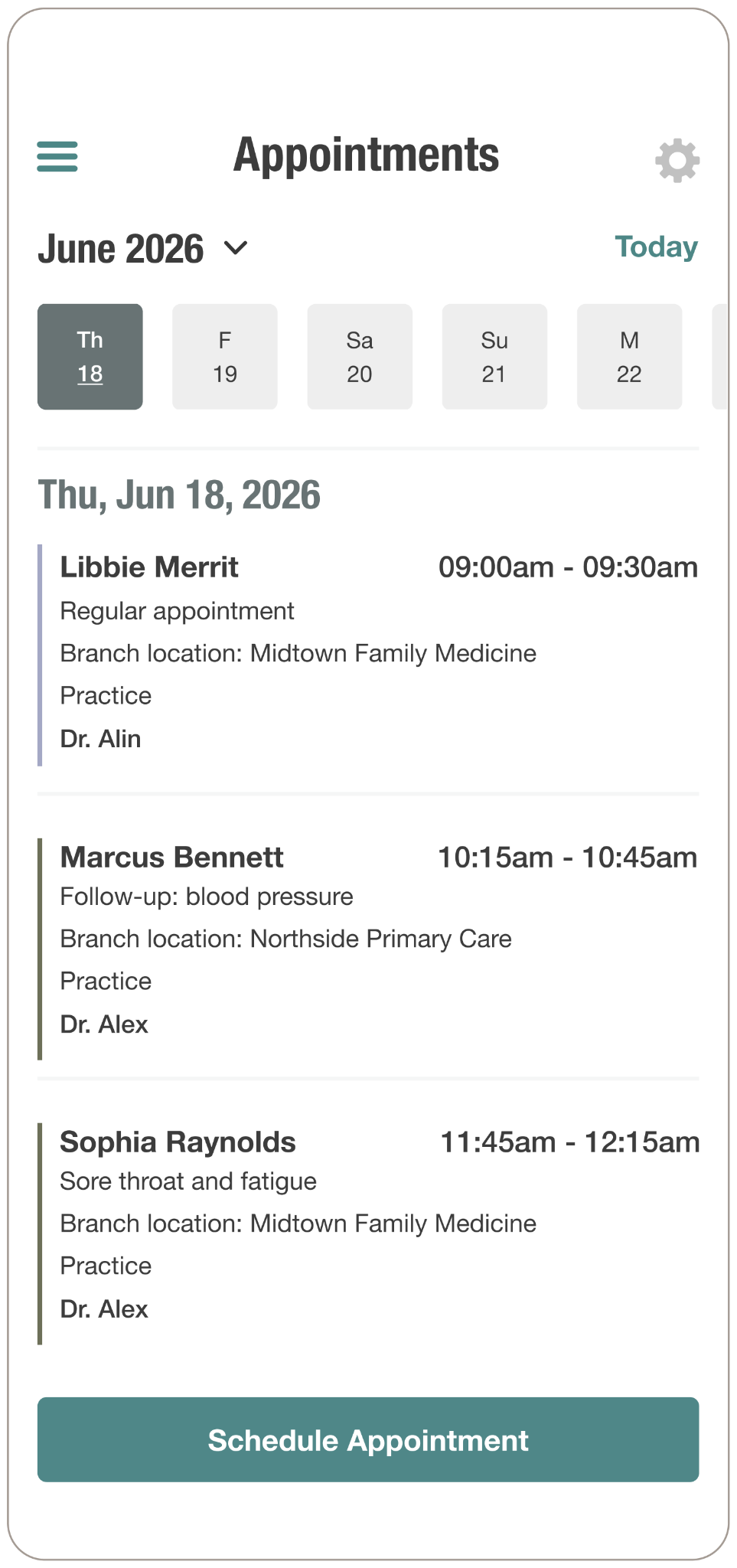
Scheduling from your phone means a follow-up appointment is booked immediately, rather than waiting until you’re back at a desk.
- Book the moment it comes up, while the patient is still with you.
- Set up the entire appointment from your phone, including date, time, patient, responsible staff member, and repeat behavior, without opening the EMR.
- Keep moving through your day, and find every appointment on your schedule when you’re back at your desk.
This isn’t meant to replace the full calendar in the EMR. It’s for the quick bookings that come up as you work, and everything you add syncs back to your schedule, so nothing slips past you.
For more information on how this feature works, check out our support article. And if you have any questions, please don’t hesitate to drop us a line at support@atlas.md.

