The American healthcare system was built around a simple assumption: most people get their insurance through their employer.
That assumption no longer reflects how millions of Americans actually work. According to the Bureau of Labor Statistics, there were 11.9 million independent contractors in their primary job alone as of July 2023, accounting for 7.4% of total employment.
Among skilled knowledge workers, the shift is even more pronounced. Upwork estimates that 28% now operate as freelancers or independent professionals, contributing roughly $1.5 trillion to the economy.
This means freelancing isn’t just a side hustle economy; it’s the new workforce, and healthcare needs to catch up.
The System Was Never Meant for Independent Workers
Employer-sponsored health insurance remains the dominant model in the U.S., covering 154 million working-age Americans. For anyone outside that system, the individual market means higher premiums, complex coverage rules, and limited flexibility.
That burden falls hardest on the self-employed. KFF research estimates that 48% of adults under 65 enrolled in individual market coverage are either self-employed, small business owners, or employed by businesses with fewer than 25 workers. For many of them, the individual market isn’t a fallback. It’s their only option.
For millions of these workers, healthcare access still feels tied to a job they no longer have.
That’s the problem Direct Primary Care (DPC) is uniquely positioned to solve. And it’s been solving it for decades.
Direct Primary Care Has Been Solving This for Decades
Long before gig work became a mainstream conversation, physicians were already building a better model.
Frustrated with the fee-for-service treadmill, a growing number of doctors began opting out of insurance billing entirely in the early 2000s, trading bloated patient panels and administrative overhead for something simpler: a flat monthly fee, a smaller roster of patients, and the time to actually take care of them.

It was a direct response to everything broken about the way primary care was being delivered. And it worked.
What’s changed since then isn’t the model. It’s the size of the population that needs it. With thousands of practices now operating in every state, DPC has spent two decades proving itself while the rest of the healthcare conversation slowly caught up.
A typical membership covers:
- Unlimited primary care visits
- Same- or next-day appointments
- Preventive care
- Chronic disease management
- Lab testing, and more
All for a predictable monthly fee with no surprise bills.
For gig workers, that structure matters in ways it doesn’t for a salaried employee with a full benefits package. Freelancers don’t get paid sick days. They can’t afford to wait three weeks for an appointment, sit in a waiting room for two hours, or get blindsided by a bill after a routine visit.
DPC removes all of that. One monthly fee, direct access to a physician, and the ability to get back to work. That kind of predictability is rare in healthcare, and for independent workers, it’s essential.
The Right Structure for Independent Workers
DPC covers the everyday, but what about the extraordinary? For major medical events like hospitalizations or surgeries, a separate insurance plan fills the gap.

The AAFP recommends pairing a DPC membership with a high-deductible wraparound policy to cover emergencies, and supplemental plans like Atlas Direct are built specifically for that purpose.
The ACA Marketplace—the government-run exchange where individuals can shop for and compare health insurance plans outside of employer coverage—is where most independent workers end up looking for that wraparound plan.
On its own, it’s an imperfect solution: premiums are high, and plans aren’t designed with freelancers in mind. But paired with DPC, a low-cost catastrophic or bronze-tier plan becomes a safety net rather than a freelancer’s entire healthcare strategy.
The result costs less, delivers more access, and actually fits the way independent workers live.
Policy Is Finally Catching Up
For years, a quirk in IRS rules treated DPC membership as disqualifying coverage, penalizing people for choosing a model that saved them money and improved their care.
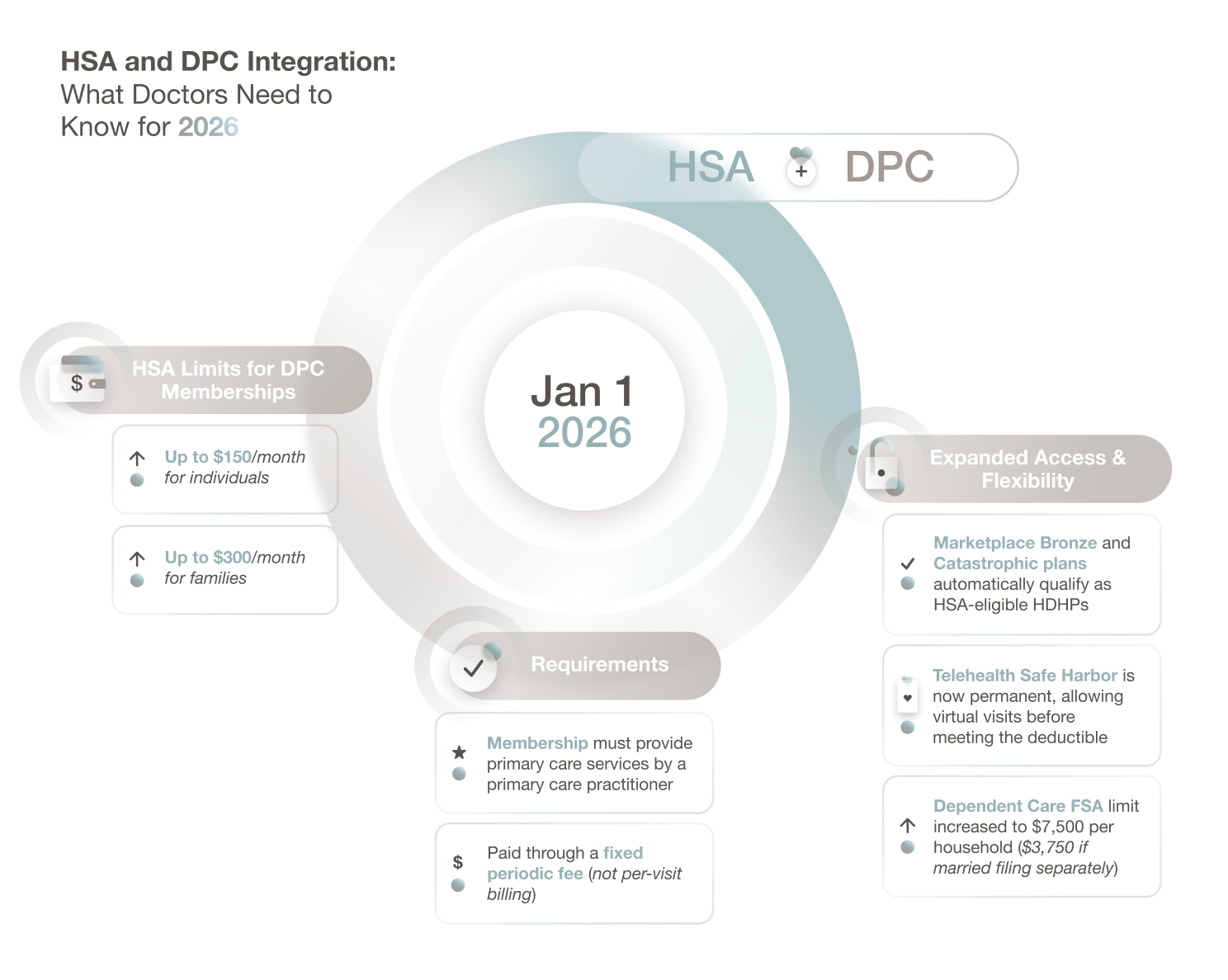
That changed on January 1, 2026. Since then, individuals enrolled in qualifying DPC arrangements can now contribute to and use a Health Savings Account.
Fees up to $150 per month for individuals ($300 for families) qualify for HSA contributions and tax-free reimbursement, making the DPC-plus-HDHP combination more financially accessible than ever for the self-employed.
The model didn’t need a policy to validate it. But removing that barrier means more people can access it.
Healthcare That Travels With the Worker, Not the Job
Work in America has changed. When nearly four out of ten workers participate in freelance or independent work, tying healthcare to traditional employment is a system built for a workforce that no longer exists.
The BLS data make the stakes clear: 80.3% of independent contractors prefer their work arrangement, yet they remain far less likely to have health insurance than their employed counterparts.
That gap is real, and it has a cost: deferred care, financial risk, and workers who have to weigh a doctor’s visit against a day’s pay.
Direct Primary Care closes that gap. It gives independent workers consistent access to a primary physician, predictable costs, and a foundation they can build real coverage around. Paired with a lean insurance plan and an HSA, it delivers what the traditional employer-based model was never designed to provide: healthcare that travels with the worker, not the job.
This isn’t a new idea waiting to be proven. Physicians have been practicing it, and patients have been choosing it. The rest of the system is finally starting to agree.